ICMR - National Institute for Research
in Bacterial Infections
आईसीएमआर - राष्ट्रीय जीवाणु संक्रमण अनुसंधान संस्थान
Department of Health Research, Ministry of Health and Family Welfare, Government of India
स्वास्थ्य अनुसंधान विभाग, स्वास्थ्य और परिवार कल्याण मंत्रालय, भारत सरकार
WHO Collaborating Centre For Research and Training On Diarrhoeal Diseases

NIRBI : Outbreak Investigations
Outbreak Investigations
Outbreak Investigation 2021 - 22
The Nationwide COVID-19 Serosurvey - Round 4 was carried out
in June 2021. ICMR-NICED, with active cooperation from the
State and respective District Health Authorities,
successfully conducted this survey in eight districts /
health districts in West Bengal - namely, South 24-Parganas,
Diamond Harbour HD, Bankura, Bishnupur
HD, Jhargram, Alipurduar, Purba Medinipur, Nandigram HD. In
each district, 10 clusters (villages / municipal wards) were
selected and from each cluster a minimum of 40 individuals
aged 6 years or more were included in this survey from the
general population. Thus, the minimum sample size per
district for the general population was 400; in addition,
100 health care workers were also included from 1 or 2
selected health care facilities. In this survey, the study
teams visited the selected households and after obtaining
informed consent, captured relevant information on an Open
Data Kit (ODK) application on mobile phones. Trained
phlebotomists in each survey team collected about 3 ml of
venous
blood from each participant. The serum was separated after
centrifugation in a local health facility and later
transported to the ICMR-NIE laboratory in Chennai. All serum
samples were tested for presence of IgG antibodies against
SARSCoV-2. Overall about 60% of the general population and
80% of the health care workers found to have antibodies
against SARS-CoV-2.
In view of rapid surge in cases and deaths because of COVID 19, deployment of Central Multi-disciplinary team was done to 10 identified states including West Bengal. The team conducted their activities for a period of five days from 27/12/2021- 30/12/2021 Assist the state of West Bengal in management of COVID-19 pandemic and worked in several districts of West Bengal to understand the situation of SARS-CoV-2 infection. To assist the state in controlling COVID-19 outbreak we visited municipal areas and blocks to access the COVID- 19 situation in Kolkata, North 42 Parganas, South 24 Parganas, Hooghly and Howrah district of West Bengal. We also visited COVID 19 hospitals, district hospitals, PHCs and diagnostic centres at Kolkata, North 42 Parganas, South 24 Parganas, Medinipur and Howrah to provide necessary support to the state. Airport preparedness was access by the team at NSC Bose Airport, Kolkata.
Areas focussed during field visit was
- Testing : RAT/RTPCR
- Contact tracing, including surveillance, containment operations
- Samples for Genome sequencing to INSACOG network
- COVID appropriate behaviour and its enforcement
- Hospital logistics: Number of beds, ambulances, Medical O2 etc.
- COVID-19 Vaccination progress
This visit was important to provide necessary suggestion for
better implementation of containment plans and micro
plans including better hospital management.

Information collection during COVID-19 serosurvey (round 4)

Specimen collection during COVID-19 serosurvey (round 4)

Specimen collection during COVID-19 serosurvey (round 4)

Specimen processing during COVID-19 serosurvey (round 4)
Outbreak Investigation 2020 - 21
to determine safety,efficacy and immunogenicitythe vaccines against SARS-CoV 2 infection like Recombinant BCG (rBCG) vaccine trial and phase III trial of the indigenous vaccine (COVAXIN). ICMR-NICED has been selected as one of the ten centres for national COVID-19 biorepositories for collection, storage and maintenance of clinical samples from COVID-19 cases for steering research in developing new diagnostics, therapeutics, vaccines against COVID-19 infection. Online systems were developed for regular communication, reporting and data generation. To support National policy and generate national level evidence, various collaborative research activities were undertaken by NICED scientists. NICED also supported basic research on Covid 19, by becoming collaborating partner with IITs and other research organizations.
COVID-19 Pandemic was the
greatest challenge of the century because of its high
infectivity and little knowledge. ICMR-NICED has been
involved in COVID 19 related activities since the beginning
of the nationwide lockdown period. With limited human
resources, mobility restrictions, the staff of this
institute took a humongous task in receiving, testing
enormous number of clinical specimens on daily basis round
the clock and providing feedback to all concerned agencies.




Outbreak Investigation 2019 - 20
Public Health Support After
Extremely Severe Cyclone "Fani" In Odisha: An extremely
severe cyclonic storm, Fani, struck coastal Odisha around
Puri district on 3rd May, 2019. Following this, several
scientists of ICMR-NICED took turn to be deployed in various
affected areas of the State as part of the Central Public
Health Team formed by the Directorate General of Health
Services, Emergency Medical Relief Division, Ministry of
Health & Family Welfare, Govt. of India to assist the State
Health Department. Dr. S. Kanungo (Epidemiologist) visited
Bhubaneswar during May 3-6, Dr. R. K. Nandy (Microbiologist)
was deployed in Puri district during May 8-21 2019, Dr. A.
K. Mukhopadhyay (Microbiologist) was posted to Khordha
District during May 8-22, while Dr. A. K. Chakraborty
(Microbiologist) was stationed in Puri District during May
23-June 06, 2019. The teams visited the affected areas and
did a rapid situation analysis, assessed the preparedness
and needs of the local health facilities especially in terms
of water and vector-borne diseases, trained several
peripheral health staff and made recommendations as
appropriate.

EMR team members and State Health Officials meeting at Puri

Filed testing for chlorination of drinking water source

Testing for Malaria parasites at the household level by EMR team using Rapid Testing Kit
Outbreak Investigation 2018 - 19
Avian Influenza outbreak
Investigation at Village Fajilkhutahari, Godda District,
Jharkhand: A Central Public Health Team was deployed by
Directorate General of Health Services, Emergency Medical
Relief Division, Ministry of Health and Family Welfare,
Govt. of India regarding Avian influenza outbreak control
and containment at Village Fajilkhutahari, Godda District,
Jharkhand during February 9-18, 2019. Dr. A. Chakrabarti
took part in the team as a Microbiologist. During the
investigation the team in association with State, District,
Block and Field level health officials. Initially the team
members were briefed by the State Headquarters and then
moved to the affected areas as per the direction. They
visited the affected areas, trained health personnels and
conducted seminar on influenza. No human cases were detected
and the situation was under control. Surveillance activity
was scrutinized and a proper surveillance was suggested.
Test laboratories were also visited and proper guidance was
provided.
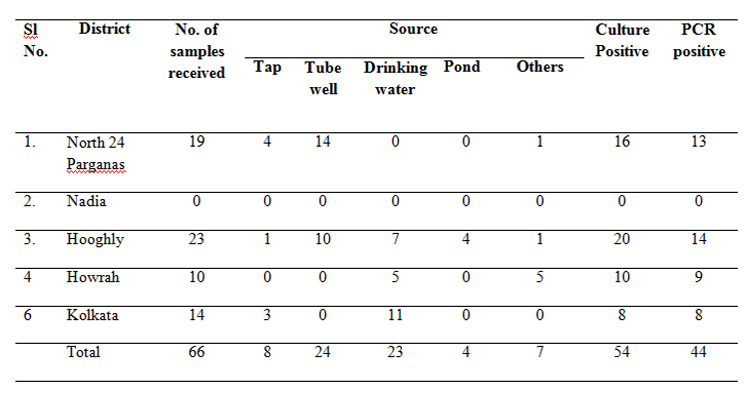
Outbreak Investigation 2017 - 18
Water samples are received from different PHCs of N. 24
Parganas, Nadia and Hooghly, Howrah, Kolkata and its
adjoining areas. Results have been conveyed to the
respective agencies with a copy of the same to State Health
secretariat, Govt. of West Bengal. During the period under
report, 66 samples had been received from various sources of
which 54 had been found to be culture positive positive (49
and 17 for the presence of faecal coliforms and V.
cholerae) (Table).
TABLE: District wise distribution of the Outbreak Water
Samples, their respective sources and organisms identified
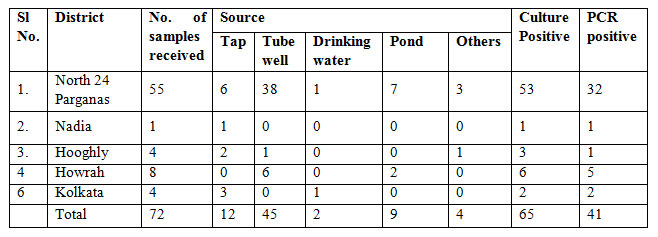
Outbreak Investigation 2016 - 17
Service provided by: Scientists of Bacteriology and Virology Division
On request from the State health referred samples from various State Govt. Hospitals were received and processed for diagnosis of dengue virus with the viral serotyping. All together around 12,000 odd samples have been screened and feedback results have been sent to the concerned department with intimation to the State Health Authority.
During the epidemic outbreaks of diarrhea which spread across different southern districts of West Bengal, microbial analysis and examination of samples of potable water sources, from different parts of West Bengal and reporting of results to the Govt. agencies, has been a routine activity of the environmental laboratory.
Water samples had been received from different PHCs of N.
24 Pargana, Nadia and Hooghly, Howrah, Kolkata and its
adjoining areas. Results have been conveyed to the
respective agencies with a copy of the same to State Health
secretariat, Govt. of West Bengal. During the period under
report, 72 samples had been received from various sources of
which 51 had been found to be positive for faecal coliforms
and 27 for presence of V.cholerae (Table 1).
Table 1: District wise
distribution of the Outbreak Water Samples, their respective
sources and organisms identified
Member of team for outbreak investigation: A.
Chakrabarti
As nominated by the Director, as per Order No
Z.28020/1/2017-EMR/AP; Dated 20th February, 2017. Dr A. K
Chakrabarti, visited Chittoor district on 24th Feb, 2017 to
investigate Seasonal Influenza /H1N1 outbreak till
01/03/2017. He was a member of the central investigation
team and investigated an outbreak of Seasonal Influenza
(H1N1) in Chittoor District Andhra Pradesh, India from Feb
24 to March 1, 2017. This visit was aimed to investigate the
situation concerning the rising trend of the H1N1 in the
state of Andhra Pradesh. The incidence of Influenza/H1N1
cases was investigated to detect the early warning signal
and trend of Influenza /H1N1 cases. Health care delivery
system of the district was assessed for detection and
management of Influenza/H1N1 cases and technical support
provided to prevent and control it.
Visited all the possible sites including District,
Municipal and regional hospitals, medical colleges around
the district and finally reported to DMHO, Chittoor District
and Secretary, State health department of Andhra Pradesh at
Vijayawada. This investigation was concluded with the report
and recommendations in a meeting with State Health
Secretary. Concerned authority of the state was suggested to
take prophylactic measure.
An Outbreak of Foodborne infection caused by Shigella
sonnei in West Bengal, India
Members of outbreak investigation team: F. Debnath, A.
Mukhopadhyay, S. Dutta, G. Choudhury, R. Narayan Saha &
Field support staff of Epidemiology division.
A total of 19 cases with acute gastroenteritis (AGE) from Pakapol village of Bhangore II block, South 24 Parganas, West Bengal were admitted to the Infectious Disease & Beliaghata General Hospital, Kolkata after having food at a housewarming party. An epidemiological and microbiological investigation was carried out by NICED team to confirm the occurrence of foodborne outbreak; to describe it in terms of time, place and person; to determine the cause of outbreak; to recommend control measures.
We carried out a retrospective cohort study among the party attendees. We collected information by using institutionally developed AGE case search format. Stool specimens from twelve case patients were processed for isolation and identification of enteric pathogens by following standard methods.
Thirty-four people attended the party on 23rd November 2016 and had lunch together. Median incubation period for development of AGE cases from time of food consumption was 18.5 hours (IQR, 16.5 -22 hours). Overall attack rate was 73% (25/34), of which 76% (19/25) required hospitalization. All age groups were affected with 100% recovery rate. One served food item was significantly associated with the illness: tomato salad (RR = 4.14; 95% CI = 1.21-14.13). Eight stool specimens (67%; 8/12) were tested positive for Shigella sonnei. PFGE analysis showed that the recent outbreak Shigella sonnei strains were clonally related with the locally circulating strains in Kolkata.
We confirmed that the food borne outbreak was caused by
Shigella sonnei and leftover raw tomatoes kept
unrefrigerated might be implicated as the source of this
outbreak.
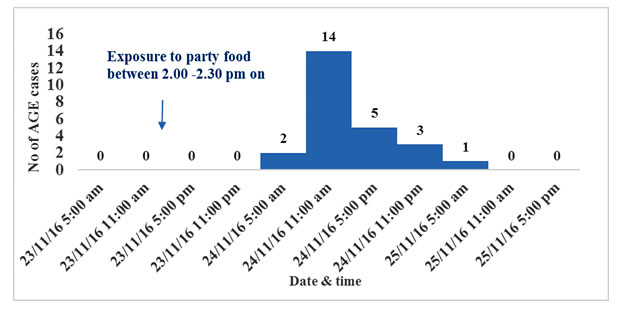
Fig 1: Distribution of Acute Gastroenteritis Cases,
food borne outbreak, Pakapol Village, Bhangore II, South 24
Parganas, West Bengal, India, 23rd - 25th November 2016

ICMR - NICED team visiting the affected family, Pakapol
Village, Bhangore II block, South 24 Parganas, November,
2016
Dengue fever outbreak investigation in Baranagar
Municipal area, 2016
Members of outbreak investigation team: F. Debnath &
field staff of Epidemiology division
During second week of August 2016, ICMR - National Institute of Cholera & Enteric Diseases, Kolkata was requested by North 24 Parganas District Health authority to carry out an epidemiological investigation at Baranagar Municipality in response to reporting of increased number of fever cases. As a response, ICMR-NICED carried out a thorough epidemiological investigation obtaining three approaches: 1) record review from local health authority 2) Door to door case search in ward no. 1 3) Case search at in/out patient department of Baranagar State General Hospital and confirmed existence of dengue fever outbreak at Baranagar Municipal area which is adjacent to Kolkata by comparing the monthly attack rate of dengue during that period to the previous three years. The outbreak started in the last week of July 2016 and continued till second week of December ,2016 (Fig 2). Total 1660 confirmed dengue cases (Over all attack rate = 7 per 1000) and two deaths (case fatality = 1 per 1000) were reported in this outbreak. ICMR - NICED, tested 212 blood specimens from probable dengue case patients of that area for confirmation through NS1 ELISA/MAC ELISA test and 163 blood specimens turned out to be dengue cases. Out of these 163 dengue cases, serotyping was done for 63 cases and DEN 1 (65%,41/63) was the major circulating serotype.
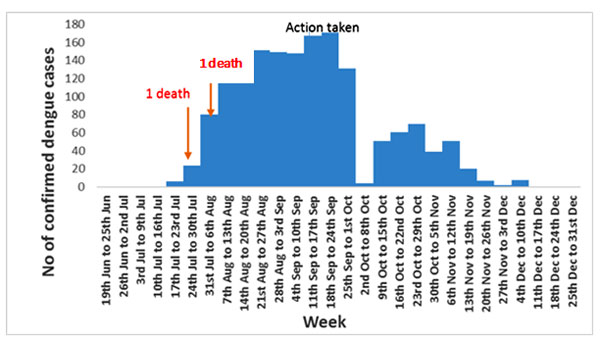
Fig 2: Distribution of dengue cases, Baranagar Municipality, July - December 2016

During training of the health workers of Baranagar
Municipality before starting house to house active case
search for dengue fever
Outbreak Investigation 2015 - 16
NICED participation in National Task Force (NTF) programme on Laboratory Containment of Wild Polio Viruses
This institute primarily works on bacterial, viral and
parasitic pathogens isolated from stool specimens collected
from diarrheal patients. Institute conducts vaccine trials
linking epidemiological findings with
laboratory based analysis in the area of bacteriology,
virology, parasitology, immunology, molecular biology and
clinical medicine. To maintain aforementioned activities, a
large number of stool specimens and/ or water samples from
diarrheal outbreak affected areas are being collected and
stored in the freezer(s) before being analyzed at NICED
laboratories. In addition, this Institute works on Influenza
virus infected specimens as and when requested by the
Ministry of Health & Family Welfare, State or Central
Government. Aforementioned all specimens as collected for
research/ diagnostic activities have been categorized under
potentially Polio risk materials by the National Task Force
(NTF) from the point of view of Laboratory Containment of
Wild Polio Viruses.
NICED actively participated in the national programme on Laboratory Containment of Wild Polio Viruses in India since its inception in 2012. Considering potential risk from the standpoint of laboratory containment of wild polio viruses special attention has been attributed for non-storage and destruction of clinical specimens like stools, water samples, and nasopharyngeal swabs and these are to comply with Phase II activity under the NTF guidelines and Global Action Plan (GAP) III protocol (2014). Institutional 'Risk Assessment and Risk Management Committee for Containment of Wild Polio P2 Virus' was formed on August 3, 2015. Since then this Institute periodically submitted containment action reports to National Coordinator, NTF. All these activities are to comply with guidelines of 'Global Polio Eradication and the Endgame Strategic Plan (PEESP) (2013-2018)'. In addition, NICED jointly with NTF, hosted a meeting on August 14, 2015 for sensitization on the importance of PEESP and this meeting was attended by several senior scientists/ head of divisions from Institutes/ Universities who are working with potentially Polio infected materials. Finally, a certification stating that NICED is not storing any potentially Polio infected materials in the freezers have been issued in April 2016.
A. Palit
Outbreak investigations (2015-16) by the Environmental
Microbiology Laboratory During the epidemic outbreaks
(2015-16) of diarrhea spreading across different southern
districts of West Bengal, microbial analysis and examination
of samples of potable water sources, from different parts of
West Bengal and reporting of results to the Govt. agencies,
has been a routine activity of the environmental laboratory
of our environmental laboratory.
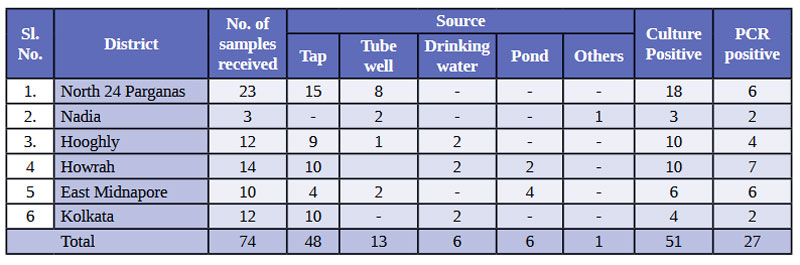
Water samples were received from different PHCs of N. 24 Parganas, Nadia and Hooghly, Howrah, Kolkata and its adjoining areas. Results have been reported to the respective agencies with a copy of the same to State Health Secretariat, Govt. of West Bengal. During the period under report, 74 samples had been received from various sources of which 51 had been found to be positive for faecal coliforms and 27 for presence of V. cholerae (Table 1).
(Table 1) District-wise distribution of the Outbreak Water
Samples, their respective sources and identification of
V. cholera
K. Sarkar
A proposal on 'Mosquito-borne surveillance to forecast any
Dengue outbreak & its control at New Town City' was
submitted to the New Town Development Authority for
necessary funding. The proposal is accepted by the New Town
Development Authority in principle and possibility of
funding is being reviewed.
Alok Deb
Investigated an outbreak along with Dr Shanta Dutta of
foodborne diarrheal illness that occurred in Sashan block of
24-Parganas (North) following consumption of offerings
devoted to the idol in a local temple during March 1-5,
2016. More than 1000 people of different age groups, who
were mostly from a particular village and consumed the
offerings made to the God in a local temple, fell sick with
diarrhea and vomiting within a few hours of its consumption.
Some of them also presented with mild fever and headache.
Around 300 people were admitted in the I.D. & B.G. Hospital,
Beliaghata from whom relevant information and stool
specimens were collected from 30 patients. A sample of the
food distributed among the affected devotees was also
received and tested.
.
Outbreak Investigation 2014 -15
Assessment of the Post-Flood Public Health Situation in Baramulla District, Kashmir during October, 2014 by NICED Scientists
The district Baramulla, located on the north-west of Srinagar, was affected by the flood later - mostly due to overflown water that submerged and created havoc to Srinagar, and in some areas due to flashfloods from heavy rainfall. The flood water also lasted only for a few days without stagnation in the affected areas.
About 16% of the villages in the district were affected by the flood. However, most of these villages were affected mild-to-moderately; some villages in a few blocks were severely affected and required special attention. These flood hit areas were already visited by one or the other EMR teams and the district health system also responded very quickly and efficiently so that the health situations even in the hard-hit areas were never beyond control.
Except for an increase in number of dermatitis cases (following contacts with polluted flood water) in some areas and an increase of road traffic accident cases noted in the district hospital, there have been no outbreak of diseases so far in the district following the flood and at present there does not seem to have an imminent threat of any major outbreak in the flood-hit areas of the district.
As far as diarrheal diseases are concerned, there was no increase in such cases since the flood - rather the number of cases in most areas showed a gradual decrease. This was possibly due to the effect of several factors - no stagnation of water, persistent use of tanker water, boiled water or water treated with chlorine tablets at household levels, as well as ensuing winter season that could negatively affect occurrence of diarrheal diseases. The other major water source to the affected areas that were being supplied through the PHE department was recently checked for adequacy of chlorination and coliform count (MPN), and as per CMO of the district, was found suitable for human consumption. Thus, there was no report of any diarrheal outbreak in any part of the district and there seemed to be no threat for any imminent outbreak of such diseases either. However, one sporadic diarrhoeal sample collected from Archanderhama of Pattan was psotive for multidrug resistant Entero pathogenic E. coli. So, continuous vigil in this regard should be maintained.
 Temporary shelters for homeless people in village Bala, Kashmir
Temporary shelters for homeless people in village Bala, Kashmir
Inspection of allocated isolation facilities for Ebola Virus Disease Outbreak by NICED Scientists during November 2014
A visit was made to STNM Hospital, Gangtok on 23 Nov 2014 by the following two members Central Team to inspect the allocated isolation facilities for Ebola Virus Disease (EVD): (Dr. Satyajit Sen, Regional Director Kolkata, Regional office of Health & FW, GOI and Dr. Shanta Dutta, Scientist F, NICED (ICMR). As per Govt. Order D.28015/4/2014/EMR/Pt from M/o Health and Family Welfare, Govt. of India, DGHS, EMR dated 21 Nov 2014, the team members started their onward journey to Gangtok, Sikkim on 23 Nov 2014. Immediately after arrival the members started visiting the different units of the Hospital e,g, Emergency, Outdoor, laboratory etc. They also inspected the under construction isolation facility of the hospital for checking the level of preparedness for EVD. The major points have been covered in the completed checklist provided by the EMR, DGHS, M/O Health and FW. Briefly, STNM Hospital has allocated one area for the isolation facilities, which may not be the ideal for construction of such unit. As per Medical Superintendent, STNM Hospital, there is acute shortage of space/ land to build such unit. The current unit has been located at least 50 meters higher up than the general hospital, and stone curved stairs need to be used for transportation of EVD patients. The unit is within the hospital campus, but attached to many other Dept. of the hospital like Cancer Registry Unit, IDD cell and Diet Stores.
Outbreak Investigation 2012 -13
During the epidemic outbreaks (2012-13) of diarrhea spreading across different southern districts of West Bengal, microbial analysis and examination of samples of potable water sources, from different parts of West Bengal and reporting of results to the Govt. agencies, has been a routine activity of the environmental laboratory. Water samples had been received from different PHCs of N. 24 Pargana, S. 24 Pargana, Murshidabad and Hooghly as well as from endemic and epidemic affected Municipal wards under the Kolkata Municipal Corporation and its adjoining areas. Results have been conveyed to the respective agencies with a copy of the same to State Health secretariat, Govt. of West Bengal. During the period under report, 45 samples had been received from various sources of which 20 had been found to be positive for faecal coliforms and 12 for presence of V. cholerae O1 (Table 1).
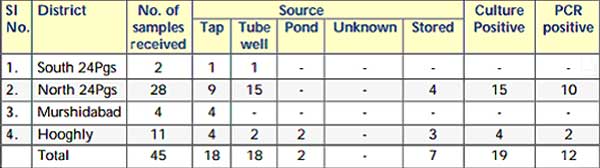 Analysis of Water/ Environmental Samples
Analysis of Water/ Environmental Samples
Outbreak Investigation 2011 - 12
Water and Environmental samples
During the focal diarrheal/cholera outbreaks (2011-12) in different southern districts of West Bengal, microbial analysis and examination of samples of potable water sources, from different districts of West Bengal as well as Municipal wards under Kolkata Municipal Corporation (KMC) and reporting of results to the Govt. agencies, has been a routine activity of the environmental laboratory.
Water samples had been received from different PHCs of N. 24 Parganas, S. 24 Parganas, Hooghly and Kolkata as well as from endemic and epidemic affected Municipal wards under the Kolkata Municipal Corporation and its adjoining areas. During the period under report, 47 samples had been received from various sources of which 39 had been found to be positive for fecal col iforms and 8 for presence of V. cholerae (Table 1).
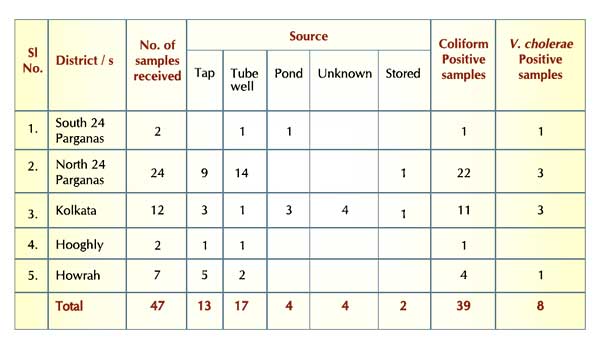 Analysis of Water/ Environmental Samples
Analysis of Water/ Environmental Samples
Outbreak Investigation 2010 - 11
Report of investigation of a cholera outbreak in Gujarat by team from National Institute of Cholera and Enteric Diseases, Kolkata, team from 31m May-2" June 2010
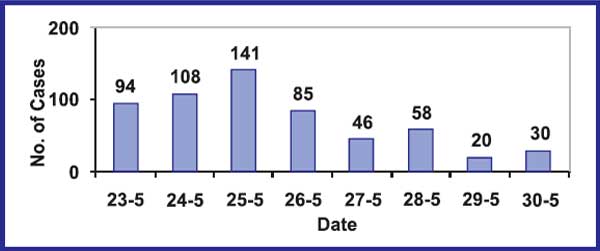
Acute Castro Enteritis (AGE) cases were reported since 23'd May from different villages of a block in Gujarat.
The week from 22nd May was marriage season during which time, there was large movements of groups of people from one village to another to attend the marriages. Most of the cases reported having attended one or other marriage ceremony. On returning to their homes, they fell ill and then spread the diseases to other members of the family. The temperatures had soared upto 48°C and there was acute scarcity of water. Since large amounts of water are required during the marriage ceremonies, water was bought in tankers from 2 open wells in Jhalod town. The wells are privately owned wells. The wells were visited by the team and were observed to be in dire state. The inside linings of the wells were not continuous with gaps in the walls where trees and other fungi and algae had grown. The water was obviously contaminated and the municipal authorities had instructed the owners to chlorinate the wells. In spite of these instructions, there was no residual chlorine in the well waters when the team tested the water with chloroscope. Instructions had also been given to chlorinate the water in the tankers but these also showed negative results for residual chlorine. Considering that the causative organism had been identified to be Vibrio cholerae, (transmitted through water), the cases mostly presented with acute watery diarrhoea with severe dehydration and the contaminated water source, it is highly suggestive of a water borne outbreak (rather than food poisoning as suspected initially). The team visited the several affected villages and interviewed some family members of diarrhoea cases. As expected, most cases reported having attended a marriage ceremony. Interestingly, there were two ladies who had attended different marriages and had only taken water but no food. They also had diarrhoea a nd stool was positive for Vibrio cholerae. This probably clinched the issue of water borne outbreak.
Laboratory report
Of 98 samples collected, 32 samples were positive for Vibrio cholerae. Antimicrobial susceptibility pattern was also tested. Of the 84 water samples sent for testing (collected from different sources of water), 50 were declared microbiologically unfit for drinking.
Recommendations advised
Most important recommendation was regular chlorination of wells and tankers supplying water to the community with routine monitoring with chloroscope for residual chlorine both at source and at the users' end.
Investigation of outbreaks of Acute Diarrhoeal Diseases (ADD)/Cholera in Rayagada and Kalahandi districts, Orissa,17-21 September 2010
At the request of the Director, Emergency Medical Relief, (EMR), Govt. of India, a team of NICER scientists went to Orissa to assist the state/ district health authorities in the investigation and control of outbreaks of acute diarrhoeal diseases (ADD)/ cholera in Rayagada and other districts of Orissa along with other experts from NCDC, New Delhi. The team visited the affected areas of Rayagada and Kalahandi districts along with senior officers from the Directorate of Health Services, Orissa and district officials during the period from 17 to 21 September, 2010.
Observations
A total of 1930 cases and 41 deaths were reported from district Rayagada in 2010 (upto 21 September). These cases occurred in 420 villages in 93 GPs of 8 Blocks. Rayagada district has reported the maximum number of cases and deaths in the state due to severe diarrhoea in 2010 (Tables 1,2)
Eight of 11 Blocks in Rayagada reported cases of severe diarrhoea in 2010. The worst affected blocks are Kalayansinghpur (704 cases, 8 deaths), Kashipur (365 cases, 10 deaths), Bisamacuttack (318 cases, 11 deaths), Jemadeipentha (269 cases, 2 deaths), Gudari (74 cases, 6 deaths) and Jagannathpur (85 cases, 4 deaths)
Analysis of 41 deaths in district Rayagada revealed that 10 deaths occurred in 6 villages of three sub-centres in Kashipur Block (including 4 deaths in village Bahardulki), 8 deaths occurred in 6 villages of two sub-centres in Ksinghpur block (including 2 deaths each in village Lekapai and Ksinghpur), and 11 deaths occurred in 6 villages of three sub-centres of Bisamacuttack block (including 4 deaths in village Gadaba, 2 deaths in village Goilkana). Thus multiple deaths occurred in some very small villages. Virtually all deaths occurred in homes (Table 1).
People were not aware of ORS, where is it available in the village and when and how to use it. Halogens tablets have been distributed in the affected areas, but most in the remote rural areas do not seem to use them in the absence of a strong IEC campaign.
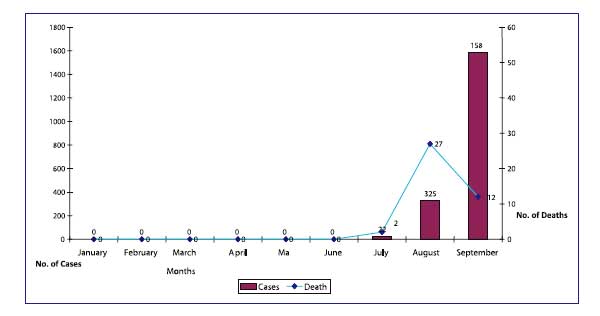 Month-wise Cases and Deaths due to severe diarrhoea in Rayagada district, Orissa, 2010 (up to 21st Sept)
Month-wise Cases and Deaths due to severe diarrhoea in Rayagada district, Orissa, 2010 (up to 21st Sept)
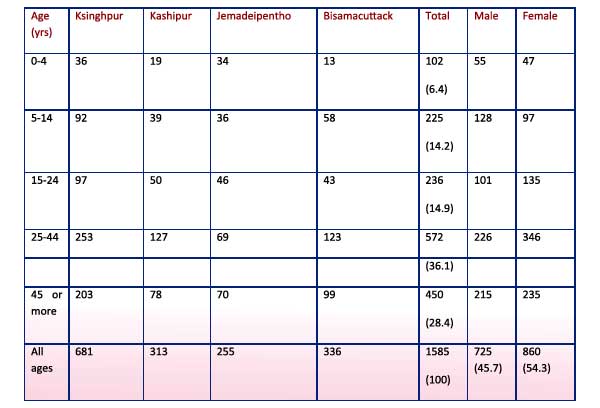 Cases of Severe diarrhoea indistrict Rayagada by age and sex, 2010
Cases of Severe diarrhoea indistrict Rayagada by age and sex, 2010
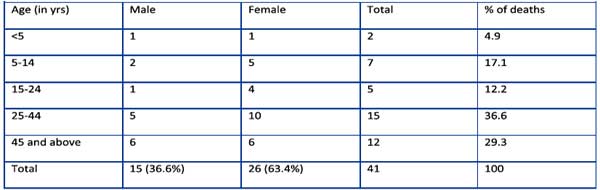 Deaths due to Severe diarrohea in district Rayagada by age and sex, 2010 (upto 21st Sept)
Deaths due to Severe diarrohea in district Rayagada by age and sex, 2010 (upto 21st Sept)
Analysis of age distribution of the deaths in Rayagada revealed that only 4.9% deaths occurred in under-five children and 78% deaths occurred in persons 15 years and above. Deaths in adults following dehydration usually indicate cholera. Male contributed to about 37% of deaths, the remaining 63% deaths occurred in females.
Clinical observations
The main presenting symptoms in outbreak associated cases are profuse painless watery diarrhoea, with or without vomiting, followed by dehydration. All these cases are managed with intravenous fluids (Ringer Lactate) and antibiotics like Norfloxacin, Ciprofloxacin, Ofloxacin and Tinidazole. None of them had received ORS at home; similarly none was given ORS solution in the treatment centre when they were being administered intravenous fluids.
Laboratory observations
During August-September 2010, 20 rectal swabs were sent to RMRC, Bhubaneswar from Rayagada district. 8 of 20 (40%) samples tested positive for cholera. The isolates were sensitive to Azithromycin, Norfloxacin, Ciprofloxacin, Chloramphenicol, Neomycin and Gentamycin. (later Ofloxacin and Doxycyclin were found to be sensitive), but were resistant to Ampicillin, Tetracycline, Nalidixicacid, Furazolidone, Streptomycin, Erythromycin, Co-trimoxazole. 14 water samples from various sources of Kashipur, Kalyansinghpur, Bisamacuttack and Gudari were also tested in RMRC, but there was no growth for Vibrio Cholerae.8 samples from district Kalahandi were also tested in RMRC Bhubaneswar during August-September 2010.5 of them (63%) were found to be positive for Vibrio cholerae 01 biotype Eltor Ogawa. 15 samples were tested in the laboratories of NICED, Kolkata. 11 of 15 samples (73%) tested positive (all Vibrio cholerae 01 El Tor Ogawa except one which was Inaba, from Kalahandi) All the 11 isolates were found to be sensitive to Tetracycline, Doxycycline, Ciprofoxacin, Norfolxacin, Ofloxacin, Erythromycin and Azithromycin; and were found to be resistant to Ampicillin, Cotrimoxazole, Furazolidine, and Nalidixic acid.
Conclusions
Clinical, epidemiological and laboratory investigations confirm the outbreak of cholera in Rayagada and Kalahandi. Although the State/District officials are making efforts to provide safe water, making the facilities available for treatment of cases and increasing awareness to improve personal and domestic hygiene to control cholera, remoteness of the affected areas and poor transport and communication facilities make the task difficult for early detection and treatment of cases which is necessary to prevent mortality.